|
In a previous post, I described what I feel to be the most important shoulder stretch. It is very important functionally to be able to reach out in front of you, and to reach overhead. While my focus in the prior post was frozen shoulder (otherwise known as adhesive capsulitis), the stretch I described is very useful for regaining function after rotator cuff surgery, shoulder labral repair surgery, and trauma. The anterior and inferior (front and bottom) shoulder capsule/ligaments are stretched using this technique. (Please note: If you are dealing with a frozen shoulder, this stretch may be too irritating to begin with. I recommend you begin with anterior, inferior capsule stretching using the best stretch for a frozen shoulder. You can come back here once you have regained the ability to raise your arm over your head again.) Sometimes, in spite of having done an outstanding job rehabilitating their shoulder following surgery, a patient may have some residual pain. Another common subset of patients presents with shoulder impingement syndrome or bursitis. These patients report pain which is usually lateral arm pain, aching in character, and may be worse at night. If forward elevation (reaching overhead), and abduction (reaching out to the side) are near normal, and rotator cuff strength is good, it is important to focus on the posterior capsule (ligaments in the back of the shoulder). A tight posterior capsule can cause abnormal shoulder mechanics. This can cause the shoulder ball (humeral head) to translate superiorly (upward) when raising the arm instead of rotating in the socket (glenoid). This pinches the rotator cuff and causes pain. The rotator cuff normally pushes down on the humeral head during rotation, but when it is irritated it will get lazy. Unfortunately, this compounds the problem, and allows the humeral head to further translate upward during activities. A cycle is then created whereby the problem gets progressively worse. We need to break this cycle. When I find the posterior capsule to be tight, I recommend using the sleeper stretch. This is a simple stretch that a patient can do on their own. As always, I recommend stretching every day, with no days off. I also recommend gentle progressive static stretching. That is, slowly applied pressure that is then held at the endpoint for relatively long duration. This means minutes rather than seconds. We are taking advantage of the viscoelastic nature of our soft tissues. The posterior capsule tends to be relatively thin tissue, and thus, this stretch does not require high force.  Posterior Capsule Stretch (Sleeper Stretch) Posterior Capsule Stretch (Sleeper Stretch) In these photos I am lying on my side. For this demonstration we will assume my right shoulder is the bad one. So, I am lying on the bad side. My elbow is out in front of me. The upper arm should be even with the shoulder. Both palms are facing toward my feet. Now gently and progressively apply force with the left hand. The goal should be to create rotation of the right palm toward the floor. This should create tension and stretching pain in the back of the shoulder. Ordinarily I would recommend resting your head on a pillow for comfort. I am not doing this to avoid obscuring the positioning.  Posterior Capsule Stretch (sleeper stretch), viewed from above. Neutral position. Posterior Capsule Stretch (sleeper stretch), viewed from above. Neutral position. Here is the view from above. Again note my upper arm is at shoulder level and my palms are facing toward my feet. Pressure is applied rotating my right shoulder internally, and pushing palms toward the floor.  Posterior capsule stretch with torso leaning slightly back. This is a less aggressive position. Posterior capsule stretch with torso leaning slightly back. This is a less aggressive position. Here is a less aggressive position. It may be good to begin this way. You can place a pillow behind your back to lean against. For all of these positions, resting your head on a pillow will allow more relaxation and thus a more pleasant stretch that you can hold for a longer time period.  Posterior capsule stretch (sleeper stretch) with torso leaning forward. This is a more aggressive position. Posterior capsule stretch (sleeper stretch) with torso leaning forward. This is a more aggressive position. This is the most aggressive sleeper stretch position. This will concentrate more force on the posterior capsule. It may not always be necessary to regain balance. I recommend testing each of this positions on the other (good) side so you have a benchmark to assess what is normal for you. Some key points:
0 Comments
In an earlier post, I described my experience with a frozen shoulder. Here are some pictures showing exactly how I rehabilitated myself and how I recommend my patients stretch on a daily basis.  The best stretch for frozen shoulder - starting position - side view The best stretch for frozen shoulder - starting position - side view The initial position will look something like this. I am using a jar of sauce to provide some downward pressure. My good arm is placed in a similar position and allowed to rest with the shoulder, elbow, and wrist touching the floor. When your bad shoulder is hurting from the stretch, look over at your good shoulder and remind yourself what normal range of motion looks like.  The best stretch for frozen shoulder - side view The best stretch for frozen shoulder - side view This is the goal. Now I am able to touch my shoulder, elbow, and wrist to the floor at the same time. You will not get to this point quickly. It will likely take hours of stretching like this over weeks to go from the first picture to this one.  the best stretch for frozen shoulder - intermediate position the best stretch for frozen shoulder - intermediate position Here is how it looks from above.  the best stretch for frozen shoulder - final position goal the best stretch for frozen shoulder - final position goal Gradually bringing your hand and elbow closer to your head will add additional stretch. Some key points:
I began playing ice hockey when I was 7 years old. When I was an orthopedic resident in New York City we formed a Hospital for Joint Diseases orthopedic hockey team. We had the unique opportunity to play outside in central park and also at Chelsea Piers with a view of the Hudson river and the New York skyline.
In spite of the violent reputation ice hockey has, I never personally sustained any significant injury. Until one evening around midnight (we had terrible ice times) when I was involved in a collision deep in my defensive zone. The back of my left shoulder made contact with the boards and I felt a zing of pain into the side of my arm. I immediately had difficulty raising my arm. Thankfully, it was toward the end of the game. I liberally applied ice when I got home, but when I woke up in the morning, I still couldn't actively raise my arm. I was fairly certain my injury was a rotator cuff contusion, and not a rotator cuff tear due to the mechanism of injury, and therefore would be self-limited. This proved to be correct, and by that afternoon, my active range of motion had returned, albeit with some pain. Confident my pain would improve as the contusion healed, I went about my normal daily activities for the next several weeks. I grew somewhat concerned however when the pain wasn't decreasing, but rather it was increasing. As a physician, working with world-renowned orthopedic surgeons who would be happy to assist me, I instead chose to ignore it. My life was too busy to deal with my shoulder. I could work, and for the most part I could compartmentalize the pain. Working at shoulder level or below was essentially normal and pain-free. But, if I forgot and suddenly reached for something, a knife-like jab brought my shoulder's issues front and center. After several months went by, I began to feel that my first choice of treatment (doing nothing) had failed. I finally examined my shoulder objectively and noted that although my strength was normal, I had lost some range of motion. More interestingly, I had lost not only active range of motion, but passive range of motion as well. At this instant I understood why my pain wasn't getting better. I had developed a frozen shoulder. Now everything made sense. At this point, I began my rehabilitation program. Everyday after work I applied ice to my shoulder for about 20 minutes. I purchased an ice machine to assist with this. I tried traditional stretching techniques, but was disappointed with the results. I was able to achieve intense pain, but absolutely no increase in range of motion. I actually felt I was getting worse. Frustration is an understatement. A possible treatment for a frozen shoulder that has been resistant to all nonoperative measures is a manipulation under anesthesia. The surgeon essentially forces the joint through a range of motion, tearing the tight tissues. This is something I clearly hoped to avoid. I recognized that biologic tissues are viscoelastic. I felt that based on this characteristic a stretch done gently, but for longer duration could be more effective. And so I began stretching differently. I measured the duration of stretch in minutes as opposed to seconds. I got to the painful endpoint and held it under tension for as long as I could tolerate it. Knowing that the longer I stretched the better it would be I increased the duration of my stretching to 30 minutes or more. Stretching hurts. I reminded myself that in spite of the pain I was experiencing, I was not creating damage. To maintain a stretch of this duration requires you to relax. The best position for me was to lay on the floor on my back and attempt to simultaneously touch my shoulder, elbow and wrist to the floor at the same time. I added some weight to my hand to increase the stretch and watched TV. I did this routine every day. At first I wasn't sure it was helping. But then I instinctively reached for something without thinking. Something that had previously caused a jolt of pain. And I felt no pain at all. This motivated me to add weight and time to the stretching program. Within a few more weeks my shoulder pain had resolved and I had regained normal range of motion. This method has made surgery for frozen shoulder very rare in my practice. When I first describe this technique to my patients, they seem incredulous. Most have already been through a course of physical therapy and are very frustrated. They presented to me to have an operation. But with very few exceptions (sometimes patients with diabetes have very resistant frozen shoulders), the vast majority of patients can avoid the operating room using this method. I will upload some pictures of how I recommend stretching in an upcoming post. Biologic tissues are viscoelastic. That means their stretchiness changes depending on how hard they are stretched. We can take advantage of this characteristic when we are rehabilitating a stiff joint. This becomes very important with certain medical problems. Specifically: total knee replacement and frozen shoulder. This concept is generally helpful in orthopedic rehabilitation and I take advantage of it whenever applicable. Think of silly putty. When slowly stretched it can be drawn out into a long strand, but when pulled aggressively it will snap and break in two. This is an extreme example of viscoelasticity. Your tissues are similar. While extreme force stretching can cause tissue to tear, this is generally far beyond any amount of stretching a patient can do, even with a physical therapist. A manipulation under anesthesia is a maneuver performed by a surgeon to rapidly regain motion in a particular joint that has become stiff. Tissues tear, and inflammation results. This is the most extreme example of a high force, low duration stretch. It is best to avoid this type of intervention if possible. It is preferable for a patient to spend the time necessary to recover joint range of motion using a long duration, low force stretch. It will result in less inflammation and less pain. Shoulders and knees commonly become stiff. Total knee rehabilitation requires stretching to regain range of motion after surgery. Stretching is required to speed up the recovery of a frozen shoulder. When attempting to regain range of motion patients are often told to stretch for 10-15 seconds and then relax. Over and over. Sometimes this is effective. Sometimes it is not. There is significant genetic variation with regard to tissue strength and inflammatory response, and significant psychological variation with regard to pain tolerance, and ability to relax while stretching. When a patient has trouble regaining range of motion I try to focus them on long duration, low force stretching. This tends to create less inflammation and is more likely to allow a patient to relax the muscles while stretching. Relaxing is very important because any muscle resistance will prevent gains in range of motion. 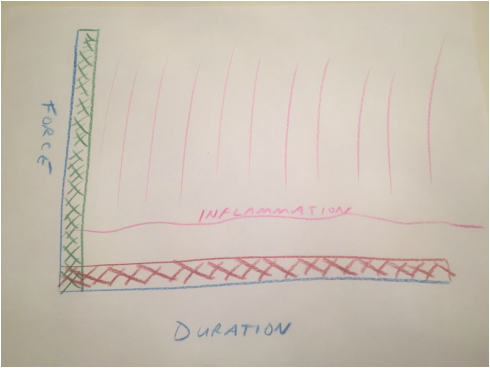 Force vs. duration stretching. A longer stretch done with less force will create less inflammation. Force vs. duration stretching. A longer stretch done with less force will create less inflammation. This sketch depicts how I think about stretching. A high force, brief stretch is more likely to cause inflammation. A gentle prolonged stretch is less likely to create an inflammatory response. The "amount of stretch" or the total area under the curve depicted by the hash marks could be identical, but my experience suggests the long duration, low force stretching will give a superior result. How do I know this? When I was a resident, I developed a frozen shoulder and used long duration, low force stretching to cure myself. I have subsequently recommended this technique to countless patients who presented with frozen shoulders that had failed to improve after many weeks of standard physical therapy. Although occasionally surgical intervention was necessary, the vast majority progressed using this technique and never needed surgery. This technique has become my standard recommendation following total knee replacement and to rehabilitate a frozen shoulder, and has minimized the need for manipulation.
|
Dr. GorczynskiOrthopedic Surgeon focused on the entire patient, not just a single joint. Categories
All
|
 RSS Feed
RSS Feed