|
A stiff total knee replacement can be extremely frustrating for patients and surgeons. The best way to manage a still total knee is prevention. I have written many articles on this website focusing on how to rehabilitate your knee replacement effectively. Unfortunately, some patients will experience stiffness in spite of their best efforts. The management pathway I have outlined below is how I recommend dealing with this problem. For a bit more explanation, check out the video posted below. 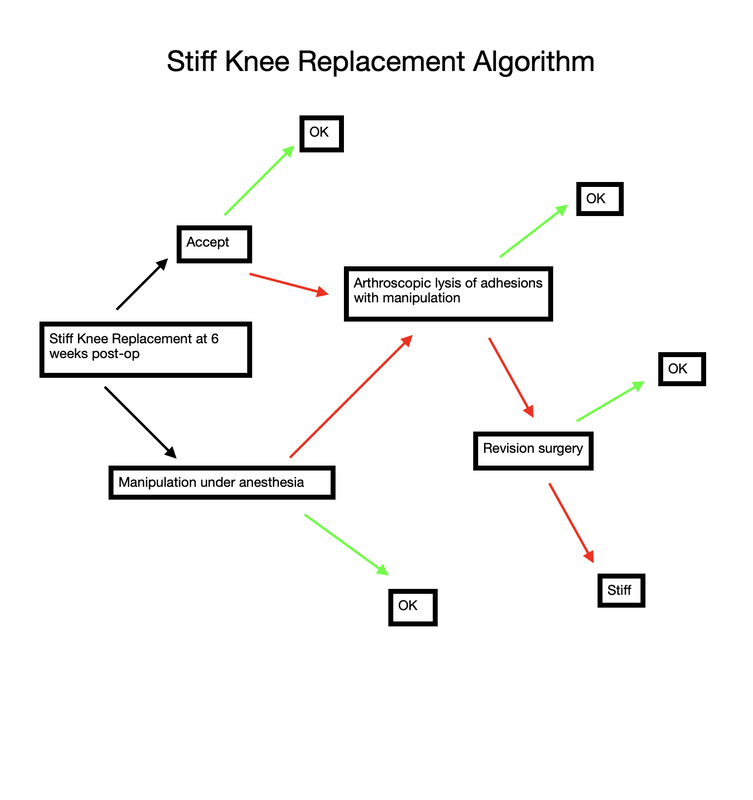 Stiff total knee replacement management algorithm
35 Comments
Uncommonly, a patient is unable to regain adequate range of motion in a reasonable period of time following total knee replacement surgery. When I observe a patient gradually falling behind with rehabilitation, I begin following them in my office more closely to provide guidance, and motivation. This can be a very frustrating situation for both the patient and surgeon. I have previously written about the tissue planes in the knee that need to be encouraged to glide, and on some stretching techniques to accomplish this. My recommendations are based in part on the viscoelastic nature of these tissues. I believe the quadriceps muscle can sometimes thwart a patients efforts to regain flexion. In the years prior to making the decision to proceed with knee replacement, a patient likely experienced episodes of giving-way or jolts of pain. The quadriceps would need to contract aggressively to prevent the knee from buckling. Additionally, many patients develop an abnormal, stiff-legged gait pattern which likely minimizes joint motion and pain. This quadriceps activity is likely subconscious, but by being repeated over a long period of time create neural pathways in the brain that are hard to break. Postoperatively, the habitual quadriceps contraction in response to pain may make rehabilitation more challenging for these patients. I have developed this idea after hearing many patients explain how hard their physical therapist is pushing on their knee, and it simply will not bend. Ive been told the physical therapist is actually off the ground being supported by the patients knee. It sounds horrible. The only way for this to be possible within the first 6 weeks or so from surgery is for the patients quadriceps to be pushing back. Guaranteed. How can I be so certain? Because of my experience with manipulation under anesthesia. At around 6 weeks from surgery if a patient and I agree that their range of motion is not acceptable I perform this procedure. A patient is briefly placed under anesthesia. I gently flex the knee while flexing the hip. Pressure is then progressively applied through the tibia and soft tissue releasing is felt and sometimes heard while this occurs. The goal is to re-establish the pre-patellar tissue plane (between the skin and the kneecap) and the suprapatellar pouch (between the quadriceps tendon and the femur). Once this has been accomplished the knee will generally flex to 120-130 degrees under the force of gravity alone. This verifies that no more joint adhesions are obstructing motion. So again, how do I know the quadriceps is fighting back? Because it only requires me to apply gentle pressure. Maybe 5-10 pounds of force. Worst case 20 pounds or so. Based on this I recommend focusing on relaxing the quadriceps while stretching. Additionally, consider pre-fatiguing them. This is a technique where you would attempt to extend your knee while blocking it from moving (isometric quadriceps contraction) Then relax the quad and enter directly into the stretch. This can create significant gains. My experience has been most positive with prolonged, low force stretching as opposed to shorter, more aggressive stretches. Relatively early manipulation of a stiff knee when necessary helps the vast majority of patients get back on track. By breaking up immature scar tissue it extends the rehabilitation window a bit. Patients still need to work hard on their stretching exercises on a daily basis, but by using this technique we can "catch them up," and help to ensure adequate function and pain relief. |
Dr. GorczynskiOrthopedic Surgeon focused on the entire patient, not just a single joint. Categories
All
|
 RSS Feed
RSS Feed