|
Total knee replacement surgery is an effective way to relieve arthritis pain when non-operative measures have failed. A substantial portion of the outcome, however, is based on adequately rehabilitating after surgery. The most important part of the rehabilitation program is regaining normal range of motion. This is easier said than done. At the time of a properly performed knee replacement surgery, the soft tissues are balanced and the range of motion should be full. That is: all the way straight, to all the way bent. This is something we test during surgery. Then the incision is closed and the healing process begins. Initially, there could be some swelling and acute surgical pain from the incision/surgical approach. Soon this acute pain subsides and stiffness begins. The stiffness is experienced by many patients as pain, especially when moving against the endpoint. In a prior posting I discussed the tissue planes that need to glide to allow proper motion. Each day that passes after knee replacement surgery, more healing occurs. This process can create connections, or adhesions, between these tissues. After about 6 weeks, enough scar tissue has formed, that most patients are unable to obtain more range of motion by stretching. In other words, at around 6 weeks from surgery no more progress with regard to range of motion is possible. The trouble is, in order to regain excellent function, adequate knee range of motion is necessary. Most patients are anxious to walk, ride a stationary bike, and are often quite focused on regaining strength. While these are fine things to do, and I certainly understand this desire, redirecting the focus to stretching appropriately remains my priority during the first 6 weeks postoperatively. Once range of motion is reestablished, all of these activities will be possible. Because we have a limited time to regain this range of motion this needs to be the priority early on. Thankfully these stretches are simple. Gently and progressively force the knee straight. And then gently and progressively force the knee bent. Simple! Except when it's not. Sometimes, and fortunately it is rare, a patient really struggles to regain range of motion after their total knee replacement. This can be a very frustrating situation for the patient and surgeon alike. I recommend stretching early, often, gently, but progressively. It is better to regain motion early than to attempt to catch up when stiffness is setting in. The simplest stretches are shown below: 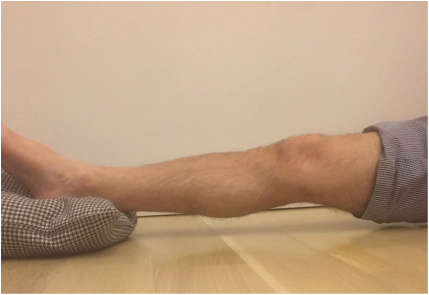 knee extension stretch knee extension stretch This is one of the easiest stretches for extension. Place your ankle on a pillow. Relax your muscles to allow your knee to sag down. Then attempt to push the back of your knee down. This is a side view of my knee. It is important to note that my kneecap and toes are pointing straight up. This stretch can be held for minutes, gradually relax your muscles more and more, allow gravity to do the work. The longer the stretch the more the viscoelastic tissues will elongate.  avoid external rotation when doing knee extension stretch avoid external rotation when doing knee extension stretch This is the wrong way to stretch. This is a view of my knee from above. There is a natural tendency to externally rotate as your hips relax. Our goals are not being accomplished if this is allowed to happen. If you find this happening, simply place additional pillows or folded blankets along the outside of your foot and thigh to hold your toes and kneecap pointing up.  knee flexion stretch knee flexion stretch Now we are working on regaining flexion. In this example we are working on gaining flexion in my right knee (in the back ground of this photo). Here I have placed my left leg in front of my right ankle. I am using my left leg to help bend my stiff right knee more. This works best when done progressively over a period of minutes as opposed to seconds. Use your hamstrings in both legs to try to flex both knees further.  deeper knee flexion test using stepstool deeper knee flexion test using stepstool For deeper flexion than the previous stretch, this position utilizes a step-stool to provide deeper knee flexion. As shown, leaning forward and applying pressure with your hands can increase the stretch.  Deepest knee flexion stretch done in supine position Deepest knee flexion stretch done in supine position This is a stretch that can achieve extreme flexion. This time I am lying on my back. My knee is pointing up toward the ceiling. Flexing the hip relaxes the quadriceps. The hands are used to to pull the leg toward your body. The effect is increased hip and knee flexion. Please note: if you have a total hip replacement, be very careful with this position as it can produce significant hip flexion. These stretching positions should take care of 90% of total knee replacement patients. These stretches should be done everyday, ideally multiple times per day, with no days off. The longer the stretches can be held, the better. Remember to relax as much as possible while stretching and remember that a little pain is normal an expected. If no pain is encountered, I would recommend pushing a little bit harder. As always, if you have any specific questions about your particular case, discuss with your surgeon.
Occasionally we encounter a patient that has a very difficult time regaining motion. I have a few additional recommendations in these cases and will address that situation in an upcoming posting.
93 Comments
Michael Rogers
10/26/2018 09:50:54 am
Dr. Gorczynski, 10/26/2018 10:22:40 pm
Tourniquet use remains routine for many orthopedic procedures. It makes the surgery a little easier for the surgeon to perform, but paradoxically may actually increase total blood loss. Like many things in medicine there are trade-offs. At this point, I recommend you use plenty of ice, continue to work on gentle progressive range of motion exercises and I am sure you will do very well.
Daniel L
11/8/2023 03:51:59 pm
Can you please discuss the pros and cons of knee flexing machines? I had my TKR on my rt knee in 2016 and I am about to have my left one done. Do you recommend the knee flexing machines? Also, I was able to achieve full extension on Rt knee but I never achieved full flexion. Is it too late for me to stretch out the flexion on my rt knee?? If it isn't which exercises do you recommend? Thanks very much - Dan 3/17/2024 07:29:41 pm
@Daniel L-
David Roberts
4/3/2020 12:45:38 pm
After having simultaneous bilateral total knee replacements, I’m in week four. 4/4/2020 12:50:18 am
This is a good technique to help regain a functional range of motion. Throughout this website, I provide some examples of more passive methods of stretching. The more you are able to stretch passively (not requiring you to exert force with your legs) the better.
Catherine Locke
6/28/2022 04:04:32 pm
I am wondering if you continue to recommend these two stretches to cover the flexion/extension. 6/29/2022 09:16:26 am
@Catherine Locke -- Yes, my recommendations for stretching have not changed. Here is a basic roadmap for recovery. This is not broken down into weekly goals as there is significant individual variation, but will provide some guidance. If you hit these benchmarks, you should be in excellent shape.
andrea
5/14/2021 11:00:29 am
I had tkr done, and I'm doing your stretches, but I'm not sure how long to hold the position that I do with my feet up on the wall and slide down. thanks.... 5/26/2021 10:38:04 pm
Stretching is most effective when done for longer periods of time. I would try to stretch in each position for at least 10 minutes straight. Total stretching time per day following surgery should be a minimum of one hour.
Susan Macaulay
5/9/2020 02:01:42 am
I am 7 weeks post-TKR (left knee). Because of the COVID-19 situation, my surgeon recommended that I attend physical therapy 2X/week for the first four weeks, and do the rest on my own at home. I suspect I may not have stretched enough during that time, because my knee is very tight, and stretching can be very uncomfortable. I've also started walking outside, and find that if I do much more than about 1/4 mile, my whole leg becomes really sore. I'm going to try to step up my stretching routine, and will keep doing the other PT exercise I was given, but am probably going to keep the walks to 1/4 mile unless I'm in less pain. (Not happy about that - I really want to begin to take the long walks I used to before osteoarthritis really took hold). Does this seem like a reasonable approach? Any other suggestions? My left leg (ankle to hip) is still noticeably larger than my right, so I'm guessing that that isn't helping things either. 5/11/2020 06:55:54 pm
Yes, this seems reasonable. Stretching is much more important than walking long distances early after total knee replacement. Walking is good, but should improve gradually with time Focus on range of motion and keep in close contact with your surgeon who should be monitoring your progress (even remotely via telemedicine).
Patricia Carver
6/20/2020 05:15:35 am
I am 5 weeks out From TKR and have flexion of 105 and 2 degrees from being straight. I have ankylosing spondylitis and prone to stiff joints. I also had damage to my knee before surgery and my presurgery numbers were 115 flexion and 10 degrees from straight. My surgeon seems happy with my numbers and hinted that I should not expect much more. I would like to achieve 0-125. I’ve been holding the longer stretches as you suggested but concerned that it is not enough and that I’m running out of time. I would be open for any suggestions and insight. 6/26/2020 06:49:40 am
I think your approach is appropriate. If you dedicate several hours each day to stretching over the next couple of weeks, there is an excellent chance you will meet your goals. Without this level of time and dedication, however, I think you may fall short since range of motion tends to become increasingly difficult to obtain as you get farther from surgery. Best of luck!
Renée Owens
12/5/2020 11:04:19 am
Thank you for sharing this information. I am 11 days out. I had a rough few days this week, and I'm terrified of the manipulation by my PT. I know it's necessary but I don't know how to make myself relax during it so that I'm not inadvertently fighting against her. Any suggestions? I feel like I'm behind and I'm trying real hard. I'm trying to do my exercises at home and i get on my recumbent bike to help push my flex and extension. How often should I be doing this? And for how long? I'm worried about the balance between not enough and too much? Finally, should I only ice or ice and heat? Ice before exercises, after or both? When would you use heat? I put heat on my hip and upper thigh today. My hip on my right side hurts from the straight sitting/ lying down position. My thigh only hurts occasionally from the exercises 12/7/2020 09:11:29 pm
Early after surgery I recommend using ice. Perhaps consider buying an ice machine to allow safe, long duration cryotherapy.
Kevin
9/11/2020 02:01:11 pm
Hi could someone give me advice please i am.a 46 year old man just found out most my cartilage worn away , however is very large with fluid, dur to lockdown im waiting to be fully assesed what can i do in the mean time i do have aspergers recent diangnosed because i was opiate dependent im now nearly 2 year clean from codiene no other drugs im finding it so hard to find someway of easing pain 9/13/2020 10:58:35 am
Until you see your orthopedic surgeon, I would recommend using ice, avoiding high impact activities, and (if you can tolerate it) over the counter anti-inflammatory medications.
Lori
9/25/2020 05:51:03 pm
Why are knee replacements clearly better in mom-opioid dependent patients? 9/25/2020 11:52:20 pm
Surgery, in general, turns out better in patients that are not opioid dependent. Multiple studies have demonstrated this. We do not know for sure why this is. But, I do have a theory. People rapidly become tolerant to opiate medications. This means that a particular dose of the drug becomes less effective over time. In addition to other medications, we also prescribe some opiate pain medication after surgery. When a patient is already tolerant to pain medication before surgery, the dose required after surgery must be significantly higher. Even then, opioid-dependent patients often have difficulty dealing with the unpleasant sensations experienced during rehabilitation. Unfortunately, poor ability to rehabilitate in the early post-operative period is likely to result in a stiffer, more uncomfortable knee.
Thank you for an excellent blog. I gound this information so helpful as I am 2 weeks post TKR. My knee is tight and swollen but as a retired
Stacey
12/7/2020 01:07:53 am
First, thank you for this blog. It’s super helpful! I am 6 days out of TKR (scope for meniscus tear 3 months ago). My physical therapist is scaring me to death by telling me I am behind in my PT only being at 68 ROM. She told me this on day 3. Is this true? I stretch several hours a day and I am honestly not in the best shape...not the worst either but gave a few pounds to lose. Do I need to be concerned or is she just aggressive in her approach? 12/7/2020 09:03:14 pm
Having surgery is stressful. I try my best to avoid increasing the anxiety level unnecessarily. The reality is that there is a limited time period during which a patient can regain range of motion. Good motion is necessary for a good result. Your surgeon and physical therapists all want you to get a great result, but they all know that rehabilitation is ultimately the patients responsibility. I think they are trying to motivate you to work as hard as you can. It is much easier to get motion back early rather than trying to "catch-up" later on. Stretching does not get easier as time goes by.
ckennedy36
12/11/2020 03:21:34 pm
I am 6 weeks out From TKR(left knee) and have flexion of 110 on my own and w/PT assistance they can get me to 117. I just came across this post this week and started holding my stretches longer than the suggested 3-5 seconds (from PT) and feeling the results/relieft already. Can you clarify that your recommendation is to work up to 10 minute holds on a stretch with a goal of getting to 30 minute hold? Right now I can hold a stretch for about 3-4 minutes. Thank you! 12/14/2020 10:36:18 pm
Correct. The longer you hold the better. I consider 10 minutes at the endpoint the minimum at this stage, with longer stretches even better. Unfortunately it becomes increasingly difficult to make progress with regard to range of motion the farther you get from surgery. This is because the scar tissue becomes more organized and stiffer with time.
gary pinder
12/17/2020 02:18:55 pm
On my 8th week and my knee is still getting stiff and swollen. The swollen goose down from time to time. As far as bending i can bend it as far my other knee.
Doug Smith
1/3/2021 10:22:41 pm
My left knee replacement 3 years ago was perfect in every way. I had my right knee replaced 4 months ago. Two days after my right knee total replacement, my knee buckled a bit while trying to stand without the walker. That is when I realized something was amiss. My knee felt like the implant would fall over a bit as I tilted my knee inward/medially. During my last PT visit, my PT doc noted that there was an unusual amount of laxity in my MCL. It's been 4 months and nothing has changed, even with all the PT exercises I do, which includes a lot of quad work. My knee clicks, clunks and catches a lot when I walk, frequently resulting in a snag that makes me squeal in pain. It's loose and feels unstable. It seems improbable that I will be able to rehab my way out of this. I wish I could get a 2nd opinion now and get this revised, but when I tried to make an appointment for a 2nd opinion I was told to call back a year after surgery. Isn't it possible to evaluate a knee replacement sooner than that to tell if revision warranted to fix the imbalance in ligaments? 1/4/2021 09:22:30 pm
I think a second opinion is appropriate. There is no reason to wait for a year. A knee replacement does not make your knee immune to injury. Most primary knee replacements require balance between the medial and lateral structures in the knee. It sounds like you may have sustained a partial tear of the MCL. At minimum this should be braced for a 6-8 week period to protect it while it heals. In the event it does not heal, and remains unacceptably lax, revision to a more constrained implant may be necessary. If your original surgeon refuses to evaluate your knee for this complaint, I would seek a second opinion.
Douglas Howard Smith
1/22/2021 03:30:48 pm
Thank you for your response. I am grateful for this wonderful service you provide. I have a 2nd opinion appointment scheduled for March 1st. I had a prolotherapy doc look at the MCL with ultrasound. All is good there. My patella tendon will hurt, pretty much all over, after a short brisk walk or just 10 minutes of slow walking on my incline treadmill. It doesn't hurt when I ride my spinner, do leg extensions, squats or wall sits. I did not have any issues with the patella tendon before surgery. Will a slightly unstable knee, such as I am experiencing, aggravate a patella tendon? 1/26/2021 11:48:00 pm
While it is possible to irritate your patellar tendon for a variety of reasons, the most common reason I see is secondary to hip weakness. Specifically hip flexor, abductor, and external rotator weakness. Check out my anterior knee pain article:
Addie Levesque
1/16/2021 02:14:27 pm
I had TKR on nov. 10th. 2 months later and I was doing pretty good. 116 rom, I think my pt said _ 2 for leg straightening. 1/16/2021 09:44:52 pm
It is hard to believe you caused much damage doing what you described 2 months after knee replacement surgery. Perhaps it was the cumulative effects of all the activity you did that day. Did your knee swell up?
Ruth Gill
2/22/2021 05:40:15 pm
I am very pleased to have found your website. I am 4 weeks post op and my knee is quite straight but also stiff. I don’t tolerate pain well but so can see I will need to do a lot more stretching!
Tracey
3/6/2021 05:58:46 am
Hi, reading all your previous replys has been informative. I'm a 53 year woman who had a left tkr 3 and 1/2 weeks ago. My extension is very good but I just can't get my flexion to go any further than a our 80. I fell year and 1/2 ago and had spiral # to my left tibia and also # tibia plateau. I was in external fixation for 6 months and had to wear a fixed brace for 3 months.My rom preoperative was flexion 50 and extension was always ok, ended up with valgus deformity. My consultant managed to get my knee flexion to 120 while in surgery. But I just cant get it to bend when in lying position any further. I'm I expecting too much to soon. My surgeon also said I might never get past 90 flexion because of the trauma. Any advice would be helpfull 3/12/2021 02:20:53 pm
In addition to the stretching recommendations I make on this website, I would ask your surgeon for a static stretching brace. Something like a J.A.S. flexion brace. This should help you maintain the stretch for long enough to at least get you beyond 90-95 degrees or so. 4/9/2021 07:10:56 pm
A friend is about to have a TKR, and is seeking my advice since I had my TKR in late November 2020. Thanks to your articles and correspondence with you I feel I have a much better grasp on the need for stretching. But would you please confirm that stretching should be started ASAP after the operation. I seem to recall your saying that a couple of days after the operation, the knee should be able to achieve 90 degree flexion simply by letting the leg hang vertically from the seated position. This seems to be a great starting point, rather than waiting one or two weeks. I cannot locate the article where you wrote this. 4/13/2021 08:20:05 pm
YES- stretch immediately after surgery, and then consistently every day thereafter. Minimum benchmarks I use: 0-90 degree arc by 2 weeks postop, 0-120 degrees by 6 weeks postop. Unless your surgeon specifically states you should not stretch for some reason, waiting 2 weeks to begin moving is, in my opinion, detrimental to a good outcome.
Merlie Aquiler
6/24/2021 03:06:49 am
I’m 5 months post op and I still have difficulty walking due to stiffness, tightness, and heaviness of my knee. I can only walk few steps and my knee starts to tighten up and pulls the muscles on my front leg and pulls down the muscles on my thigh. My surgeon told me honestly that he does not know what’s going on with my knee. I had an MUA 6 weeks after my surgery. My ROM now is 125-135 and 0 extension. I got to PT 3 times a week. What do you think is going on with my knee. I want my life back! 6/28/2021 12:48:14 pm
This is not a typical outcome for a total knee replacement. I am not able to definitively diagnose this in this format, but if your surgeon is stumped, I would recommend you seek out a second opinion. It is normal to experience improvement for an entire year or so following knee replacement surgery, but your symptoms do not sound normal for the excellent range of motion you describe.
Merlie Aquiler
6/28/2021 01:55:41 pm
I went to see another surgeons (2 surgeons) and they can not find something wrong with my knee. They both said I need more time to heal because my knee got traumatized both from surgery and MUA. My incision has keloids and it’s still sensitive and I get pain that stings (burning). Hoping my knee will heal soon and able to walk normally.
Kathy
7/18/2021 07:38:56 am
I am 10 weeks post op from TKR and about 2 weeks ago my scar tissue developed a hard knot which I assumed was just scar tissue but it has not gone down and now hurts underneath especially when I bend my knee. I went to the surgeon and he said there is no infection and is probably from the suture dissolving. It does not feel like fluid – feels very hard. Anyone else have this and if so, did it go away?? I keep massaging as if it is just scar tissue but it has not helped. My husband says it looks like an alien is about to pop out! Very ugly too. Any help is appreciated. 7/28/2021 08:46:20 pm
This sounds like a reaction to absorbable suture material. This sometimes results in inflammation, occasionally creates a localized infection called a suture abscess. It usually will resolve with time, sometimes requires some antibiotics. If it does not resolve in a reasonable time period, it is reasonable to excise the inflamed tissue and re-close this area using non-absorbable suture material, which is less reactive, that would then be removed in a couple of weeks. 7/19/2021 10:03:12 am
I am 10 months out from a left knee TKR. Since three months out I have had swelling and pain in at the lower outer knee. (It would be Florida on the map.). I was at first told it was my IT band, that from my hip to my knee it was tight. After two months of exercise nothing changed, including the swelling. At eight months, I had another visit and the doctor indicated ( after checking the area) that it was probably tendinitis of the patella. I realize some stiffness around the band is likely to always occur, and it doesn’t hurt so I can live with it. However the swelling on the outer right portion of my knee, if touched, is still very painful and I can’t seem to obtain an answer from the doctor except “it hasn’t been six months yet”, and now “it hasn’t been one year yet”. I have a high tolerance for pain and am told my range of motion is “excellent”. I have woken up from sleep in excruciating jabbing pain, until I can move my knee into a position where it feels like it “pops back”. I have had two x-rays and told my alignment is excellent. Is an MRI in order? I can do all my exercises, and they do not hurt. It only hurts if my knee is moved toward the right. I cannot sleep on my right side because the pressure pulling on this area truly hurts. It has not gotten better since this pain began at three months out, no matter what advice I’m giving to try. It does not seem to me that it is a bone issue, but more a tendon or nerve issue. Any ideas? 7/28/2021 08:36:50 pm
Your result is definitely an outlier. When a patient continues to have pain in their knee beyond the usual postop expectations, I agree that an MRI scan is in order (with metal artifact reducing sequences) in an attempt to explain the symptoms. Unfortunately many times we are not able to definitively diagnose complaints like yours, but the good news is most of these things do gradually resolve given enough time and proper rehabilitation. The main purpose of the MRI, in my opinion, is to rule out stress reaction.
Dave R
7/23/2021 03:58:19 am
Thank you very much for this site! The articles and information on it have been very helpful. I have one question which I haven't seen covered - hopefully I didn't miss it. I had a right knee TKR 8 weeks ago and seem to be doing fairly well with my recovery so far. I am completely off the prescription pain meds, and am now only using acetaminophen and ibuprofen occasionally. The pain and swelling continue to decrease, though I still have some. Currently, after some gentle stretching exercises, my ROM is 0° - 132°. This is not achieved by pushing the joint externally, but with my own muscles. 7/28/2021 08:13:00 pm
This is an excellent question. Most modern knee replacements use fixed bearings. This means the polyethylene spacer is solidly fixed to the tibial baseplate. Deep flexion will absolutely NOT cause it to pop out. There are some mobile bearing implants where the poly can move a bit on the tibial baseplate. Usually, there is a built in motion limiter, for example a post the engages into the baseplate. This allows rotation but prevents translation. If you have a posterior stabilized knee replacement, there is a post built into the tibial component that engages with the femoral component to prevent posterior translation of the tibial component relative to the femoral component. In certain circumstances a patient with this kind of prosthesis that regains deep flexion, and attempts to simultaneously tries to kneel or otherwise experiences posteriorly directed force to the tibia could "jump the post." Perhaps this is what your PA was thinking about. This is a serious, but thankfully rare complication. In my opinion, it is not something that a patient should artificially limit their range of motion to try to prevent though. The best advice I can give you is to aim for a functional range of motion. Motion that allows you to do the things you want/need to do. Forcing more just to "get a better number" does not make sense to me.
Dave R
7/30/2021 10:16:28 pm
Thank you very much for taking the time to answer my question. During my follow-up visits, the time in the exam room with the PA is fairly limited. He's good about answering my questions but, due to my very scant knowledge on the subject, I have limited ability to counter, in order to gain answers that completely satisfy my curiosity. Your answer above gives me everything I need to proceed with my recovery in confidence.
Kellie
8/26/2021 08:48:04 am
Should I just power through pain/fear/thigh muscle tensing and force ROM beyond my comfort zone? I’m terrified of injuring myself by forcing ROM but my window is closing for ROM and I’m only at 70degrees ROM when PT assists. I had MPFL recon surgery w/,donor MPFL and loose cartilage removal arthroscopy 5 weeks ago. 9/1/2021 03:56:43 am
In general, I would recommend increasing the duration of stretch as opposed to simply pushing harder. If your surgeon would consider manipulation under anesthesia around 6 weeks if your range of motion is inadequate, then you really don't need to fear injuring yourself at this point because significantly more force would be applied at that point compared to anything you could do to yourself by stretching.
Doreen Woodford
12/12/2021 12:38:01 am
I had a TKR 5 weeks ago. My range of motion is at 110 but my biggest issue in increasing it is intense focused pain in the centre of my buttock approximately I/3 of the distance from my waist to the bottom of my buttock. My quads seem relaxed. I've brought this up with my physio, but they haven't made any suggestions. It is really holding me back as this pain kicks in before I reach my "endpoint" and discomfort persists after finishing the stretch. 12/16/2021 03:44:12 pm
This sounds like sciatica. I recommend that you discuss this with your surgeon.
I had a TKR about 1 year ago and had a joint infection about 2 weeks after the surgery. My surgeon opened the knee up, performed a debridement and replaced the spacer. I completed a 6 month antibiotic therapy and blood test were done to make certain that the infection was gone. 12/29/2021 08:57:55 am
Unfortunately, you experienced a rare, but severe, complication of joint replacement surgery. Without knowing more about your knee function at this point, it is not possible for me make prognostic determinations. However, your knee withstood significantly more trauma/inflammation than the typical knee following knee replacement surgery. This may account for some stiffness/discomfort, relative to normal expectations.
Kim
1/19/2022 10:56:55 pm
Thank you! Appreciating all the info here. I am 59 and 10 weeks out. My question/situation: my flexion seems to be decreasing! I was at probably 170 last week and very happy think maybe I will be able to sit on my heels again . ... but now I’m having pain run down my tibia. and I’m maybe 140 max. My PT says I have shin splints and need to walk less. But I have a pocket of inflammation just above my peroneal nerve and I’m thinking nerve pain or inflammation. 1/22/2022 01:04:13 pm
170 degrees of flexion is supra-physiologic. If you currently have 140 degrees of flexion, this should be very near heel on buttocks, and you will be in the top percentile of outcomes following total knee replacement. It is unusual to develop new shin pain during the normal total knee replacement recovery. If you have been very active/walking for long distances, I agree with the recommendation to reduce this activity a bit, but I would also recommend a low threshold to having your surgeon check you out. It is important to rule out a stress fracture if this shin pain does not rapidly improve.
Lori Kragnes
2/22/2022 02:10:23 pm
I had a total knee replacement 5 weeks ago.My quadricep has not fired since surgery..They actually kept me in a brace for 5 days so that has set me back on my range of motion.do you have any suggestions for quad not working. I cannot lift my leg and I have been on a walker since surgery. 2/26/2022 02:50:01 pm
This is not normal. I would recommend EMG/Nerve conduction testing at this point to help understand why your muscle is still not firing.
Lori Kragnes
2/26/2022 03:13:37 pm
Thank you so much. I see my surgeon on 2-28 and I will request some testing to be done. It's still not firing.
Lori kragnes
6/27/2022 11:15:06 pm
I wanted to let you know that I did end up having an EMG a nerve conduction test they found that I had severe femoral neuropathy. I cannot seem to get an answer of how this happened but I do know that the nerve will grow back hopefully however on May 15th I had a slight movement and liftedmy leg 3 inches. This is a good sign,each day I'm getting stronger and stronger. Do you know how fast this nerve is to regrow? I'm almost 6 months out from my tkr and do you know how this could of happened. They say it may be the tourniquet but the operative report does not show anything unusual with the tourniquet being on to long that would of caused femoral nerve damage 6/29/2022 12:22:25 pm
While it could be related to the tourniquet pressure setting during surgery, it is most likely just a bizarre, fluke occurrence. Typically once recovery begins, we believe a nerve will recover at the rate of about 1 millimeter per day.
Lori Kragnes
2/26/2022 04:05:19 pm
I had a tkr on January 20,2022. I recently wrote to you regarding another issue. My other question to you, is it normal to have a knee immobilizer placed on my leg after surgery ,in which it stayed on for 5 days, which was my 1st appointment with the PT but actual PT was done 2 days later. So regardless that my quad did not wake up, My ROM is 55 degree. 5 weeks and 2 days since surgery. 4/9/2022 07:02:26 pm
I do not place patients into an immobilizer after knee replacement. I would like to see range of motion 0-90 (minimum) by 2 weeks, and 0-120 degrees by 6 weeks postop.
Lori Kragnes
5/8/2023 01:52:26 pm
Hi doctor,you were nice enough to respond to all my questions last year regarding my tkr and I ended up with severe femoral neuropathy however I wanted to give you a short update of my situation. I did end up with femoral neuropathy and due to no movement in my leg for 6 months after my total knee replacement I ended up with a quad that had a trophied.I am still in PT a year and a half later very limited range of motion and still walking with the cane very fluke thing that this would have happened but again no one seems to know what happened in that operating room and why I ended up like this.My range of motion is at 108 and the straightening is lacking three degrees I am still trying to do steps. I've worked very very hard to get back some strength. My question to you; do you know how long a nerve has before it actually shuts off any more regrowth? It's been 1 years and 5 months, so I'm thinking it can't grow back anymore. 6/20/2023 07:35:32 pm
I think after 18 months or so, a nerve injury is considered permanent. That being said, assuming you have some motor function, you should be able to regain strength for much longer, perhaps several years. 5/31/2022 03:00:56 pm
I like how you said to do stretches. My aunt is needing to get a total knee replacement done. I'll pass this information along to her so that she can know more about recovering.
Tonia Thibodeau
7/21/2022 03:21:33 pm
Hello, I had a TKR on left knee 6 weeks ago and cannot get past 100 degree flexion forced. I have a problem with keloid scarring so I am thinking this is what is happening . I am 1.5 weeks out from my Dr's. appt where he will probably recommend manipulation but I am having so many other knees problems that I am not sure manipulation is the right course or will the keloid scars just return. I have already had such a hard 6 weeks. My Therapist has no idea what is causing these issues. I am having Popping and Clicking on the inside of the knee with walking and exercises that is very uncomfortable. I am constantly stiff, the moment I stop moving the knee and recently and the most painful is it feels like something is twisting within the knee. Its not the knee cap but in that area. I read your article about planes getting stuck and I wondered if this is what is happening? When this happens it is very painful and I cannot bend my knee without extreme difficulty because its as if something is not aligned right. Any thoughts or insight you have on these issues would be very helpful. Thank you. 7/29/2022 07:34:43 am
A stiff total knee will feel like it is binding. It may be painful, swell, and feel like a tight band is constricting it. It is best to prevent this through early, consistent stretching as I describe throughout this website. Once it is stiff and you are beyond 6 weeks from surgery, manipulation is sometimes required. It is crucial to consistently stretch your total knee replacement every day for long periods of time to maintain as much of this regained motion as possible.
Nora Ramos
9/1/2022 07:41:22 am
Hello, I’ve had R- tkr on July 25, 2022. I get PT 2x a week, 9/6/2022 04:01:14 pm
You bring up an excellent point about anxiety.emotions holding you back. Your body has undergone a stressful, traumatic experience. It releases stress hormones to help deal with this. Experiencing pain, and feeling pressure to rehabilitate properly, all while having some questions/concerns about the healing process can difficult to deal with emotionally. It is important not to let this get in the way of your rehabilitation, however. While you may not feel like you have control of the outcome, you do have control of the steps you take each day to get toward your desired outcome. Throughout this website, I describe how to rehabilitate properly. If you simply do your best to stretch on a daily basis, use ice to help reduce inflammation, and do your best to make gains between formal physical therapy visits, you should end up with a nicely rehabilitated total knee replacement. Aches, pains, and stiffness will get better for an entire year. Check out my article on numbness lateral to the total knee incision, and how that is totally normal. 9/7/2022 09:48:08 am
I am 1 week post partial right knee replacement. Trying very hard to do my stretches 6 times daily. I am currently at 105 degrees flexion. I am concerned about the pain I have from the occlusive dressing. It feels like my skin is ripping when I stretch, and that is what is holding me back. I wonder if this has been a problem for anyone else. The dressing will be removed in 1 week, but I feel I would make more progress if I didn’t have a burning , ripping sensation when I stretch. Your thoughts? 9/7/2022 12:19:14 pm
If you feel your dressing is binding, and preventing you from stretching as far as you'd like, I would recommend lifting the dressing and adjusting it so that it is no longer stopping you from stretching. Allowing the dressing to reduce your ability to rehabilitate is not ideal. Also, stretching against the dressing could cause your skin to blister. Neither of these options makes sense to me. A quick call to your surgeon's office should allow you to confirm they are ok with this plan as well. If this was my knee, I would absolutely loosen the dressing to allow proper range of motion.
Joyce
10/6/2022 03:06:37 pm
Hi, Very frustrated person here!! I am almost 6 post op after a knee replacement. I caught covid after going to PT first visit. Couldn’t go for 2 weeks to PT (Hospital rules). Now I’m very behind because I didn’t feel good enough to do much stretching during that time. I’ve been doing my stretching exercises 3 times a day now for 3 weeks I’m having to fight the swelling resulting in extreme tightness. I’m at 95/0 and apt Monday with surgeon. Numbers aren’t high enough I’m told and might have to have a MUA! Don’t want that, what else can I do???? 10/23/2022 10:55:41 pm
Unfortunately there is no shortcut- long duration, frequent stretching with ice and NSAIDS is really the only way to improve range of motion. If unsuccessful, MUA is a good backup plan.
Mary
2/14/2023 12:08:51 am
I had total knee replacement surgery on January 12th. My extension is at 3 and my rom is at 108. I have been stuck at 108 for 2 weeks. I’m not sure how to get either my extension or rom more. I go to PT 3 days a week. Do you have any suggestions on what or how I can do to achieve this? I’m getting worried because I will be 5 weeks from surgery on February 16th. Thank you for all the advice that you. 2/16/2023 10:18:26 pm
Stretching is dose dependent. This means that longer duration stretches done more frequently will result in improved range of motion when compared to shorter duration, less frequent stretching. So, if you are not progressing, you are not stretching with a high enough dose. Increase your frequency, duration, or (ideally) both. You really should be stretching for a least an hour cumulatively every day, and perhaps even more, considering where you are in the recovery period.
Linda G Taylor
2/16/2023 11:32:42 am
I am day#2 post-op TKR. Knee is understandably very stiff. I am doing ice, leg raises, and calf pumps. Is it too soon to begin the stretching? I would hate to go.through all this and not get great rom! Thanks. 2/16/2023 10:15:18 pm
It is definitely not too soon to begin stretching. Generally, patients that get range of motion back early, do better throughout the entire course of rehabilitation, and ultimately end up with a better functioning, less painful knee.
Kathy Rexrode
2/17/2023 09:29:19 am
I had TKR in May 2021 and recently when I stand up from sitting I hear a “Velcro tearing” sound in the knee. The knee is very sore after that happens - some slight pain but not horrible. I hear the sound worse if I put my hand on the thigh area right above the knee to assist in standing up. Is this normal and is there something I can do to stop it and help it not be so sore? Thanks. 3/4/2023 12:30:35 pm
I wrote an article about this issue. Copy and paste this into your browser.
Steven Channick MD
2/20/2023 11:56:05 pm
Dear Dr. 3/4/2023 12:37:55 pm
I think full extension is possible, but will require dedicated, long duration extension stretches. I think weighted prone hang is one of the most powerful methods. Machines will over-estimate your range of motion due to soft tissue deformation. I believe this accounts for the discrepancy you have observed. Your surgeon could also order you a JAS extension brace. This is a static stretching device that allows you to progressively push your knee into greater extension AND THEN HOLD IT THERE, for a long duration. This is the key. Your soft tissues will need to be slowly drawn out and then maintained in the fully stretched position to allow them to adapt/accommodate.
Kathy
3/4/2023 08:40:33 pm
I had a TKR on my left knee back in 2018 and for about the last year or so have been having pain in that knee, especially while walking up a hill however I can walk up stairs fine. My surgeon stated he could replace the plastic spacer. 3/23/2023 04:00:53 pm
Unfortunately, there is not a standard presentation for a loose prosthesis. If your knee was doing well for several years and only recently has become intermittently painful, that is concerning. I am not sure what exchanging the polyethylene is intended to do for your problem. If the pain is mostly after a long walk, this seems more consistent with a stress reaction. I think your complaint requires a very careful physical examination, and scrutiny of x-rays/bone scan. It is also important to rule out an infection using labs, a joint aspiration, a white blood cell scan, and also consider metal sensitivity workup. Unless the diagnosis is severe polyethylene wear, I would not recommend simply having a polyethylene exchange. 3/11/2023 02:42:09 pm
This is a great article on how to rehabilitate your knee after a total knee replacement surgery. As someone who has had this surgery, I can attest to the importance of rehabilitation and regaining normal range of motion. The stretches provided in this article are simple and easy to follow, and I appreciate the emphasis on stretching early and often. It can be tempting to focus on regaining strength and mobility, but without adequate range of motion, those goals become much harder to achieve. I also appreciate the cautionary note about external rotation during knee extension stretch and the reminder to be careful if you have a total hip replacement. Thank you for sharing this valuable information! 3/28/2023 12:46:20 pm
Hello Dr Gorcznski, 5/7/2023 03:32:40 pm
This is a very unusual complication following knee replacement surgery. The most likely reason is pain inhibition. This is when the quad involuntarily contracts less when the knee is sore. It would not be under volitional control. Think of the instantaneous withdrawal reflex when you accidentally touch a hot stove. I would expect this to improve with time/healing. It could be a result of bruising from a tourniquet that may have been used during surgery. This, also, should simply improve with time. It has been several weeks since you wrote this comment. Hopefully your problem is resolving as expected. If it has not, perhaps you and/or surgeon should consider electrophysiologic studies to make sure the nerves that supply your quadriceps are working properly. 5/8/2023 12:49:47 pm
Thanks for your explanation. Have confirmed a tourniquet was not used during my knee replacement surgery. Currently, at 9 weeks post Left TKR and there has been improvement since I first posted on your website. After 5 more weeks of intensive PT, my Quad Lag is now 5%-10% off full function (from approximately 50%.) So, I’ve been able to transition from the walker to a cane. And the past few days, I’ve been walking without a cane using it only when my leg is sore or if I’m walking outdoors. Flexion has now reached 140; Extension at 0.
Dave R
7/7/2023 01:09:00 pm
Dr Gorczynski - 11/4/2023 11:38:38 pm
Anterior knee pain is a common affliction for many people. If can affect anybody including patients after knee replacement surgery. This is usually exacerbated by stairs, hills, and prolonged sitting with the knees bent. It almost always at least partly the result of weakness around the hips. This is where the most attention should be spent. Here are some simple exercises to focus on. Your comment will be posted after it is approved.
Leave a Reply. |
Dr. GorczynskiOrthopedic Surgeon focused on the entire patient, not just a single joint. Categories
All
|
 RSS Feed
RSS Feed