|
With over a million knee arthroscopic surgeries performed in the United States every year, at this point just about everyone has heard about someone having their knee "scoped." This is a quick, low risk procedure that provides relief in the majority of patients. Why then am I finding myself spending increasing amounts of time talking patients out of this procedure? It is important to understand what can be done to a knee with the arthroscope.
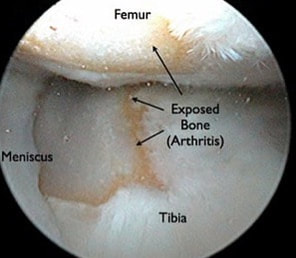
It is crucial to understand one very important thing that can NOT be done with the arthroscope. We can not "remove," "clean-up," or otherwise fix arthritis. Arthritis involves the permanent loss of articular cartilage. This is the cartilage cushion that coats the bone ends as they meet within the joint. Once articular cartilage is gone, it is gone. The solution when symptoms are unacceptable is joint replacement. Not arthroscopy. So what does all of this have to do with the meniscus? Let me describe an extremely common situation I encounter in my practice. A patient presents to my office with chief complaint of "torn meniscus." They have already had an MRI scan done. Indeed, contained within this report there is reference to a "meniscal tear." There is often reference to some degree of chondromalacia, articular cartilage degeneration, exposed bone, bone marrow edema, or subchondral cysts. All of these terms are essentially saying: "osteoarthritis." I always look at these MRI images with patients. I describe all of these pertinent findings. I explain that when there is arthritis in the same knee compartment as a meniscal tear, the pain is most likely due to the arthritis. Even if the meniscus is contributing to the pain, removing it will in no way guarantee pain relief. Many times at this point I am then asked, "so can you clean up the meniscal tear?" It is this fixation on the meniscus that I am attempting to correct. It is crucial to understand that surgically treating a degenerative meniscal tear in an arthritic knee is unpredictable at best. A patient anticipating a miraculous cure can easily be disappointed with the result.
 Standing knee x-rays may reveal joint space narrowing. This finding is consistent with arthritis. Arthroscopic surgery to address the meniscal tear in such a situation is likely to be disappointing. One of the most important studies we do is standing knee x-rays. Bone partially blocks x-rays whereas cartilage does not. When standing, a healthy knee has a clear separation between the femur and tibia. This separation is known as the joint space. It shows us how much articular cartilage there is. This joint space is not the meniscus, it is articular cartilage. When this joint space becomes narrowed, we know there is some arthritis. The term "bone-on-bone" arthritis refers to the complete loss of joint space on a standing knee x-ray. This is what severe arthritis looks like.
A good candidate for meniscal surgery is a patient who has been experiencing ongoing pain, swelling, and who has tenderness to palpation over the involved joint line. This is usually made worse by crouching or twisting. Standing x-rays should not reveal much, if any joint space narrowing. An MRI scan should not show articular cartilage loss or bone marrow edema. In this situation, a knee arthroscopy is a low-risk, high-reward procedure.
4 Comments
PAULA FREDERICK
2/8/2018 02:59:33 pm
Excellent article. Excellent physician
Caroline Thorley
7/23/2020 02:47:32 pm
Very inciteful article and helpful information on meniscus tears and explaining how and why surgery can/ won’t work 1/20/2024 01:22:43 pm
I had arthroscopy 6 years ago for a chondral full thickness fissure at the posterior superior medial femoral condyle as well as small free edge tears of both the medial and lateral menisci. Since then arthritis has progressed to now advanced state. I am doing everything possible to avoid TKR including all the different shots up to and including umbilical stem cells and RFA 7/20/23. Recently I've done extensive ROM therapy but nothing seems to work at maintaining ROM with the best results being extension of 12 and flexion at 120. I've read all of your articles about the importance of ROM by 6 weeks post TKR. Although I did PT following knee arthroscopy six years ago to "clean up" the fissure flap and tears in both meniscus, I was not warned about the importance of maintaining ROM. Is my decreased ROM since that procedure 6 years ago a muscle and tendon problem that can be corrected, or is it a result of the arthritis evolution to its advanced stage now. If I do have to get TKR, won't I need 0 and 130 ROM prior to in order to get full ROM following TKR? Is the diminished ROM I have now from the arthroscopy and arthritis correctible since it's been so many years since I had the arthroscopy surgery. It seems that the gains i get from long stretching therapy goes right back to bent the next day. I've been trying to get it to go straight thru therapy and home stretching for six months now. My stem cell doc tells me to keep at it but I'm beginning to give up hope that extension will ever get to 0 and stay that way. 😫 3/17/2024 07:49:51 pm
Losing range of motion is very frequently a part of the progression of osteoarthritis. This is not generally something you can prevent by stretching. You do not need full range of motion prior to surgery to get good range of motion after surgery. My sense is that your arthritis has progressed to the point that motion loss is becoming obvious to you. If your joint space has narrowed, your range of motion is decreasing, and your quality of life is negatively impacted, perhaps you are nearing the point of requiring joint replacement. If this is ultimately a choice you make, your surgeon should be able to restore nearly full range of motion during surgery. Then, focus on regaining full range of motion as soon as possible after surgery. I thoroughly describe how I recommend doing this throughout this website. This should leave your knee in good shape for decades. Best of luck to you! Your comment will be posted after it is approved.
Leave a Reply. |
Dr. GorczynskiOrthopedic Surgeon focused on the entire patient, not just a single joint. Categories
All
|

 RSS Feed
RSS Feed